Confident Ambiguity
I currently work with a large percentage of patients who experience “complex ” and/or “chronic pain”. Many have multiple surgical intervention histories (most repeat surgeries), every known non-invasive treatment (multiple episodes of PT/chiro/body workers), and every known pharmacological intervention known to man. All of these patients share a similar story, they were all told that “X,Y,Z” would resolve their pain or dysfunction with absolute certainty, everyone told them it was a simple fix. Yet, here they are continuing in pain, or in worse pain, in front of me.
As I sit back and review many of these cases, the most consistent theme I see of why they continue to suffer is that the traditional differential diagnosis has failed them. Many were told they had a specific diagnosis and were given a specific treatment. Differential diagnosis is based in the contemporary utilization of “Occam’s Razor”, which is the principle that “Among competing hypotheses, the one with the fewest assumptions should be selected.” (Side note: Historically it has been argued this statement is an inaccurate reference to Occam and was created by later philosophers) . Utilization of Occam’s razor is critical to many aspects of healthcare, in particular emergency medicine. However, regarding pain, it is a principle which falls far short. Pain is complex, not simple.
The absolute, “this tissue/disease is the issue”, which is both culturally and healthcare driven, is why we are in a chronic pain epidemic.When it comes to pain and movement, physical medicine and rehabilitation professionals need to come to terms with the complexity of pain. It is never a single factor, even if there is a single predominant source of nociception. This also holds true for acute injury, you must account the environmental factors and the processing, as well as the outputs:

Louis Gifford’s Mature Organism Model – 1998
This understanding makes pain and movement complicated, it makes things a bit gray, there is no absolute. You must make a clinical decision to guide the treatment, you need to be able to identify red flags quickly, you need to identify some important tissue issues, but you also must be able to confidently proceed with fair degree of uncertainty with a great deal of grace and skill. I call this skill, “Confident Ambiguity”.
Confident ambiguity allows a clinical decision to be made in the absence of an absolute diagnosis, and the absence of absolute certainty. Classically, you would look at it as a list of possible diagnosis, within your differential, but now you are asked to not just identify the possible biomedical diagnosis but also the psycho-social factors and assume for all of them to be present concurrently with a constant dynamic shift, as well as combined presence, in any given moment (Louis Gifford calls it the “Shopping basket”).
Research and clinical prediction rules help, but they need a larger framework to address all the concurrent layers of a biopsychosocial model. Personally, I, as well as many others, have been drawn to Ronald Melzack’s work on the neuromatrix at face value to help with developing a constant confident inventory of inputs/outputs in the biopsychosocial model. At all times, while interacting, assessing, and treating, in the back of my mind I play the “input/output” game, which at first appears challenging, but over time is very re-assuring both for yourself and your patient based on the dynamic nature of the interaction. This same approach has been beneficial with performance enhancement.
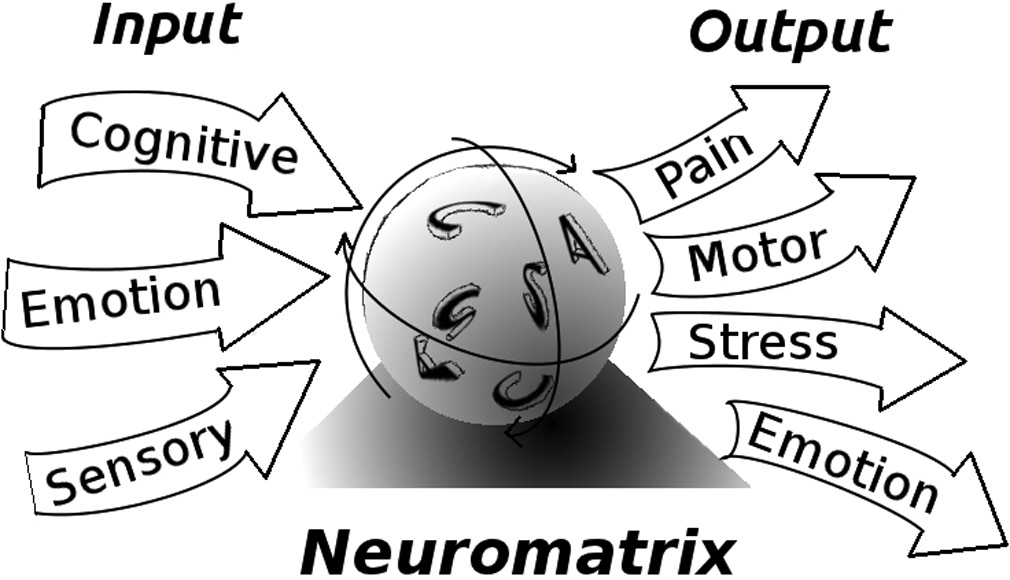
Melzack, Ronald and Joel Katz. “Pain in the 21st century: The neuromatrix and beyond.”Psychological knowledge in court. Springer US, 2006, 129-148
Every pain experience and every movement dysfunction cannot simply be broken down to single tissue damage, single disease, length tension relationships, muscular imbalance, tissue restriction, or any other musculoskeletal emphasized diagnosis. You must learn to accept the fact that the tests you delivered ,which you so confidently felt were reproducible to a specific tissue or movement pattern, may at least in part be a “neurotag”, a pain and/or movement memory that is driving everything you see and feel.

Furthermore, lumping the patient into a primary “psychosocial” driver of pain is a also problem, one cannot ignore sensory input, regardless of whether it is nociception or any other sensory input perceived as a threat.
Pain is complicated, pain is messy, if we don’t treat it as such, you will be lost and you aren’t give the patient everything they need.
Leave a Reply
Want to join the discussion?Feel free to contribute!